

Normal ABG Interpretations

Arterial blood gases (ABG) are a quick way to evaluate for respiratory, circulatory, and metabolic disorders. ABGs are ran from an arterial blood sample and give you the following results: pH, PaCO2, PaHCO3, PaO2, base excess/deficit, and SaO2. If you are a bedside nurse working in an area where ABGs are commonly drawn, you should know how to quickly interpret ABG results, as well as what they mean and how you might fix them.
Why is your patient’s CO2 elevated? What can you do to fix this? What might your nursing assessment look like in a patient with a low HCO3?
Allen’s Test
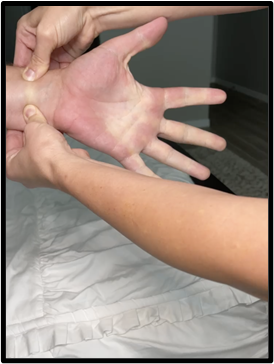
An Allen’s test is a quick way to identify if a patient has adequate arterial circulation in their hand prior to puncturing the site for an ABG (or arterial line). To perform this test:
- Locate the ulnar and radial arteries on your patient’s hand.
- Occlude both arteries and have your patient clench and open their hand 10 times
- Release the ulnar artery and maintain radial artery occlusion.
- The hand should flush pink. Capillary refill time should be less than 6 seconds in order to have a POSITIVE Allen’s test.
*If capillary refill time is greater than 6 seconds, this indicates a NEGATIVE Allen’s test and that circulation may be compromised if intravascular access to the artery is initiated
Metabolic vs. Respiratory
When interpreting an ABG, it is important to note if it is a metabolic and/or respiratory issue. So, how do we know if we are looking at a metabolic or respiratory issue?
If PaCO2 is the cause, it’s RESPIRATORY! If PaHCO3 is the cause, it’s METABOLIC! If both are the cause, then you have a MIXED respiratory/metabolic issue.

Three Easy Steps to ABG Analysis
Interpreting an ABG can seem complicated at first, but trust me, once you get the hang of it…it is easy peasy! Here are three easy steps to analyzing ABGs:
- Always assess the pH first! Is it normal?
- Is there acidosis or alkalosis?
- Which other value is trending with the pH? PaCO2 or PaHCO3?
*BONUS TIP: remember “ROME” (Respiratory Opposite Metabolic Equal)
- If the pH and CO2 are opposite: REverse = REspiratory
- If the pH and HCO3 are both up or down: saME = Metabolic
Compensated

A compensated ABG demonstrates that the patient’s body is compensating for the abnormal value driving the pH. If the pH is NORMAL and PaCO2 and/or PaHCO3 are ABNORMALl, then the patient has a compensated ABG.
For example:
pH 7.36 (normal, but on the more “acidic” side)
PaCO2 48 (abnormal…RESPIRATORY)
HCO3 24 (normal)
The interpretation of this ABG would be a compensated respiratory acidosis.
Uncompensated

In an uncompensated ABG, the pH is ABNORMAL and either the PaCO2 or the PaHCO3 are ABNORMAL.
For example:
pH 7.26 (acidosis)
PaCO2 55 (respiratory)
HCO3 24 (normal)
The interpretation of this ABG would be uncompensated respiratory acidosis.
Partially Compensated
In a partially compensated ABG, the pH is ABNORMAL and the PaCO2 and PaHCO3 are both ABNORMAL (but leaning in opposite directions…aka one leans acidic and one leans alkalotic).

For example:
pH 7.30 (acidosis)
PaCO2 58 (elevated..would cause acidosis)
PaHCO3 30 (elevated..but would cause alkalosis)
Partially compensated ABGs always confused me, but think of it this way…
The body is trying to compensate for the “off” pH, but it hasn’t quite made it all the way. If your CO2 is driving the acidosis, the HCO3 will try to become more alkalotic to “balance” the pH.
Mixed
Mixed ABGs may be the easiest to recognize, because BOTH the PaCO2 and PaHCO3 are driving the pH up or down.

For example:
pH 7.16 (acidosis)
PaCO2 60 (acidosis)
PaHCO3 12 (acidosis)
This would be a mixed acidosis.
OR
pH 7.56
PaCO2 27 (alkalosis)
PaHCO3 (alkalosis)
This would be a mixed alkalosis.
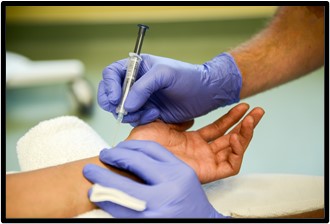
Three Important Factors When Drawing ABGs

When drawing an ABG, it is important to remember these three factors in order to ensure your results are accurate!
- Samples should be analyzed quickly! Ideally < 30 minutes
- Your heparin syringe is balanced to run electrolytes
- An Allen’s test is done prior to radial puncture
Did you know that you can run electrolytes on ABG samples?!?
Normal Venous Blood Gas (VBGs) Values
Venous blood gas results are slightly different from ABG results! It is important to recognize this in the event that a venous sample is accidentally drawn or your provider intentionally orders one. Here are the normal VBG values:
- pH 7.32-7.42
- PaCO2 38-52 mmHg
- PaO2 28-42 mmHg
- PaHCO3: 19-25 mmol/L
- SaO2: 50-70%

Being able to recognize these subtle differences between ABGs and VBGs are critical for making clinical decisions. Have you ever accidentally drawn a VBG? It happens quite frequently since the radial artery and vein are so close to one another.



Add comment