


ScvO2 and SvO2: What is the difference?
ScvO2 stands for the “saturation of central venous oxygen” and is a surrogate to SvO2. SvO2 is considered the “gold standard” for most places but it can only really be measured with a PA catheter.

Both of these measurements measure the mixed oxygen saturation of the blood. Essentially, how much oxygen is “left” after oxygen is delivered and consumed by the cells/tissues. That little “c” in ScvO2 stands for “central,” meaning that the blood sample was taken centrally (such as from a central line). A normal SvO2 is 60-80%, and a normal ScvO2 is typically higher at 70-85%. In normal circumstances, you can anticipate the ScvO2 to be slightly higher since the measurement is taken in the superior vena cava vs. the pulmonary artery; Therefore, less oxygen is delivered to the tissues at this point.
There are four factors that affect SvO2/ScvO2: cardiac output, hemoglobin, oxygenation, and oxygen consumption.
This concept still can be really confusing so think of it this way:
A red blood cell delivers 30% of its oxygen to the tissues/cells prior to reaching the heart. If you drew a ScvO2 from the patient’s central line, you would anticipate it to be 70% because 70% of the oxygen was “left” bound to the red blood cell.
If your ScvO2/SvO2 are lower, this means oxygen demand/consumption is HIGH.
Knee Mottling
We have all seen it. That super septic patient whose skin begins to mottle…and we all know what it means…NO GOOD.
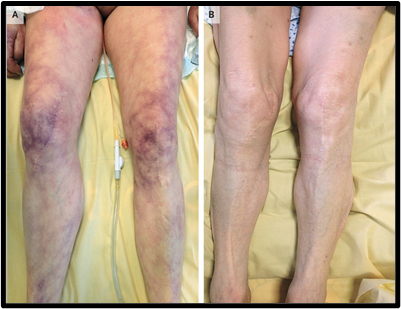
But really…skin mottling, and more particularly, mottling over the knees, is independently associated with in-ICU mortality! In one study, the in-ICU mortality rate of patients who had persistent skin mottling, no matter what their organ dysfunction was, was 40%.
Does anyone else find this fascinating!? Despite all of the fancy gadgets we have for monitoring patients in septic shock, knee mottling is a solid predictor of patient mortality.
Check out the article here.
Perfusion Assessment
We cannot talk about hemodynamics without talking about performing a solid perfusion assessment. Of course, all of the fancy hemodynamic monitoring gets us all hyped up, but there are many ways you can assess a patient’s overall “hemodynamic stability” without having them hooked up to any devices. Here are some components to include in your perfusion assessment:

- temperature
- heart rate/pulse
- blood pressure
- skin color
- cap refill
- pulse oximetry
- urine output
All of these components tell you one thing…is your patient perfusing their tissues/organs? If one of these areas is abnormal…why? Is there a good reason? Is there something we can do to fix it? Do we need more invasive hemodynamic monitoring to identify specifically what may be going on?
All of these components tell you one thing…is your patient perfusing their tissues/organs? If one of these areas is abnormal…why? Is there a good reason? Is there something we can do to fix it? Do we need more invasive hemodynamic monitoring to identify specifically what may be going on?



Add comment