

What Are Hemodynamics?

Hemodynamics measure the basic cardiovascular function of how well the body is perfusing. To put it in simple terms, hemodynamics measure how well the heart is pumping, how much fluid is in the cardiovascular system, and how well the arteries and veins are holding up.
When nursing students/new nurses hear the word “hemodynamics,” they are often intimidated. In this blog post, we will be breaking down each component of hemodynamics to hopefully make them less scary.
Purpose of Hemodynamic Monitoring
What is the purpose of hemodynamic monitoring? Do we monitor hemodynamics on every single patient?
In short, yes! As bedside nurses, we are constantly observing and assessing patient’s hemodynamics through non-invasive measurements, such as blood pressure, cap refill, heart rate, etc.
When it comes to more invasive monitoring, the purpose of hemodynamic monitoring can be for a multitude of reasons:

- Evaluation of fluid responsiveness
- Evaluation of medication administration
- Detection of life-threatening conditions (like cardiac tamponade or heart failure)
- Assess cardiovascular functioning
Invasive vs Non-Invasive Hemodynamic Monitoring
There are several ways we can monitor a patient’s hemodynamics. Depending on your facility, you may have more (or less) of these options available to you. Hemodynamic monitoring can be divided into three categories: invasive, minimally invasive, and non-invasive. Here are a few examples from each category that you may have heard of:
- Invasive: central lines, pulmonary artery catheters, esophageal dopplers
- Minimally invasive: arterial lines (FloTrac sensor or Acumen IQ sensor)
- Non-invasive: Bioreactance (Cheetah), ClearSight, ultrasound technologies
The use of minimally invasive and non-invasive hemodynamic measurement devices are on the rise. Invasive monitoring, although sometimes necessary, poses increased risk for infection, complications, and is more expensive. The reliability of minimally invasive and non-invasive measures has improved dramatically over the last several years, so you may see these monitoring devices popping up more frequently in your hospital.
Preload, Afterload, Contractility
Preload, afterload, and contractility are the three basic components that make up hemodynamics. Over the next few posts, we will be discussing each of these components in detail. But, here is a quick summary of each for your reference:
- Preload = VOLUME
- Afterload = RESISTANCE
- Contractility = SQUEEZE
Each measurement we discuss will have a “right sided” measurement as well as a “left sided” measurement.
Preload: CVP and PAOP
Preload refers to the end diastolic volume. There are two main measurements of preload that are commonly used in the ICU world, one for the right side of the heart and one for the left:

- Central Venous Pressure (CVP 2-6 mmHg): CVP measures the volume of blood in the vena cava, which is near the RIGHT atrium of the heart. A low CVP would indicate that there is less volume entering the heart. The difficult part about CVP is that there are so many factors that influence it (vascular tone, intra-abdominal pressures, intrathoracic pressures, blood volume). Anything that changes your intrathoracic pressure, such as increased PEEP levels on the ventilator, can change your CVP. This is due to the fact that increasing PEEP decreases your venous return. CVP is a useful tool as long as its limitations are understood, but should not give any direct indication of left heart filling.
- Pulmonary Artery Occlusive Pressure (PAOP 6-12 mmHg): PAOP measures the volume of blood entering into the LEFT atrium. It is most commonly measured by performing a “wedge” with a pulmonary artery catheter; However, this is a practice that is phasing out and may not be used in your facility due to its risk for rupturing or perforating the pulmonary artery. Instead, many units will rely on the pulmonary artery diastolic (PAD) pressure as a nearly identical measurement to the PAOP, as long as a patient’s heart rate, blood pressure, cardiac output, and overall clinical state remain stable.
Afterload: PVR and SVR
Afterload is the measurement of RESISTANCE in the blood vessels (think vasoconstriction and vasodilation). In other words, afterload is the impedance the ventricles must overcome to eject its blood volume. Afterload is influenced by: size/wall thickness of the ventricles, volume ejected, and impedance of the vasculature. There are two measurements of afterload we look at: SVR (left ventricle) and PVR (right ventricle)
- Systemic Vascular Resistance (SVR: 800-1200 dynes-sec/cm^-5) measures the resistance the left side of the heart has to overcome in the systemic vasculature.
- Pulmonary Vascular Resistance (PVR: <250 dynes-sec/cm^-5) measures the resistance the right ventricle has to overcome to push blood through the pulmonic valve.
Contractility: Ejection Fraction
Contractility is the heart’s ability to contract (go figure LOL), aka squeeze. It is the inherent property of the heart’s muscle fibers to shorten, independent of preload/afterload. A good measurement of contractility is ejection fraction (EF).
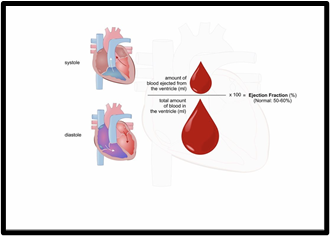
A normal EF is typically 55-70%. EF measures the percentage of blood pumped out of the heart at the end of systole. For example, an EF of 60% would mean that 60% of the blood was pumped out of the heart, while 40% remained. Typically, the EF refers to the EF of the left ventricle (LVEF), but we can also measure the EF of the right ventricle (RVEF).
A lower EF may mean there has been damage to the heart’s muscle (heart attack, cardiomyopathy, etc). An EF less than 40% may signal heart failure.
Stroke Volume/Stroke Volume Index
Stroke volume is the amount of blood (in mL) ejected from the heart with each beat (60-100mL/beat). Stroke volume index is the same measurement, just based on a patient’s body surface area (BSA). Stroke volume is one of my favorite hemodynamics because it is a good indication of fluid responsiveness (check out our past post on passive leg raise). It also is affected by all three components of hemodynamics: preload, afterload, and contractility.
Increased preload = increase in stroke volume
Increased afterload = decrease in stroke volume
Increased contractility = increase in stroke volume
Cardiac Output/Index
Cardiac output is the amount of blood (L/min) ejected from the left ventricle in one minute. It is calculated by multiplying the patient’s heart rate by stroke volume (CO = HR x SV). Cardiac index is the patient’s cardiac output divided by their body surface area. Cardiac output can be influenced by anything that impacts a patient’s heart rate and stroke volume.
Stroke Volume Variance (SVV)
Does your patient need volume? Let’s check out their stroke volume variation (SVV)!
Wait! What?? I thought stroke volume variation was not an actual predictor of preload?

Correct! While SVV is not an indicator of actual preload, it has been shown to be a very sensitive and specific indicator of relative preload responsiveness.
SVV is the difference between maximal stroke volume and minimal stroke volume during respiration. Literature supports using SVV with patients who are 100% mechanically ventilated (no spontaneous breathing), and who do not have arrhythmias. Normal SVV values are typically less than 10-15% with controlled mechanical ventilation. A SVV greater than this could indicate a need for more fluid.
In summary, SVV is a fantastic tool to manage fluid responsiveness as long as it is used within its limitations! Check out this great article on SVV and its use to improve hemodynamics.
Importance of using BSA
BSA (body surface area) is the measurement of a person’s body surface area. For medical purposes, BSA is a more accurate indicator of metabolic mass. In order to calculate a patient’s BSA, you must know the patient’s height and weight.

So, why is this important? Let’s look at cardiac output. A normal cardiac output is typically between 4 to 8 L/min. But, let’s say you are taking care of a patient who is 5 ft tall and another patient who is 6 ft tall. Do you think these patients will have the same cardiac output? Most likely not. We would anticipate the 6ft tall person to have a higher cardiac output than the 5ft tall person.
If we calculate their cardiac index, which is cardiac output divided by a patient’s BSA, we can get a more accurate, specific measurement for that patient. For example, if the patients above both had a cardiac output of 4 L/min, this might be too low for the 6 ft tall patient if calculated by using BSA. Even if 4 L/min is “within normal range” for a cardiac output, it may not be within a normal range for cardiac index for someone with a higher BSA.
Frank-Starling Law
Does the phrase “Frank-Starling” bring you back to your nursing school days? So, what is it?

The Frank-Starling Law is the heart’s ability to change the force of contraction in response to volume status. In other words…
The more blood in the vascular system, the more the heart has to stretch to compensate for the extra blood; Therefore, a bigger force (contraction) will occur.
My favorite visual analogy for this is a water balloon. Think about it…the more water inside a water balloon, the more the water balloon has to stretch. The more water inside will create a greater force of ejection when the balloon is popped.
Add comment