
Indications for Emergent Pacing
Over the next few weeks, we are going to be chatting all things related to emergent pacing!! When it comes to emergently pacing your patient, it can be a bit intimidating…but we want to break it down and make it EASY for you. Let’s start with a few indications for emergent pacing:
- Symptomatic bradycardia
- Complete heart block (3rd degree)
- Second degree type II heart block
So, just remember…when your heart is racing because you need to do some emergent
pacing…your patient’s heart rate is going to be LOW.
Types of Emergent Pacing
There are three types of emergent pacing:
- Transcutaneous
- Transvenous
- Epicardial

All of these methods are temporary measures until a patient gets a pacemaker, or the issue for pacing is resolved.
Single Chamber Pacing vs. Dual Chamber Pacing

Single chamber pacing vs. dual chamber pacing….What’s the difference?
In single chamber pacing, only the atria or ventricle is being paced. This is usually done with transcutaneous pads OR a pacing lead in the right atrium or right ventricle.
In dual chamber pacing, both the atria AND ventricle are being paced. Dual chamber pacing requires two leads, and is typically done with epicardial wires.
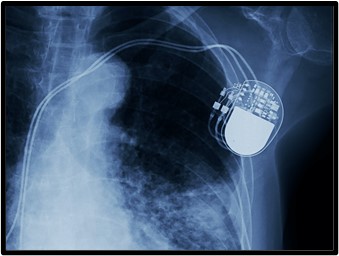
Pacemaker Codes
VVI, DDD, AAI….OH MY! Pacemaker codes can be so confusing…so let’s break it down.
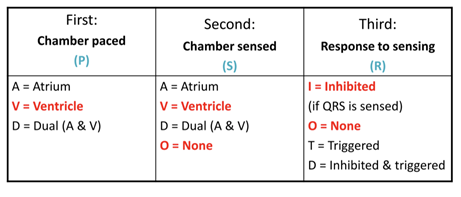
-The first letter = chamber paced
-The second letter = chamber sensed
-The third letter = response to sensing
Transcutaneous Pacing

Transcutaneous pacing (TCP) is done via pads that are placed directly onto a patient’s skin.
These pads are the same as the ones you use during codes to “shock” patients and are typically found on your code cart, pacing cart, or in the supply room. It is important that you know where your transcutaneous pacing supplies are, though, because transcutaneous pacing usually happens very quickly when a situation warrants it.
TCP is a non-invasive form of emergent pacing that is not as efficient as transvenous pacing. It requires more energy (most adults will need a minimum of 50mA) because it is done through electrodes placed onto the skin.
TCP is a temporary method of pacing to stabilize a patient until a more permanent method can be accomplished. As you can imagine, this type of pacing is not very comfortable to patients who might be awake (as their CO improves so will their LOC)…so sedation or analgesia may be needed.
Pad Placement Prep

Before you transcutaneously pace someone, it is important to make sure the the pads are properly placed and adhered to a patient’s skin. Here are a few pad placement tips:
- Make sure the skin is clean
- Clip excess hair
- Ensure pad is completely adhered to the skin
- Anterior/posterior placement preferred
- Place pads 2 inches from permanent pacemaker
Demand vs. Asynchronous Modes

It is VERY important to know the difference between demand and asynchronous modes when it comes to pacing a patient.
In demand mode, pacing only happens when needed. The patient’s intrinsic activity is detected and pacing is inhibited when activity is sensed. This mode is overall safer for patients.
In asynchronous modes, the pace rate is programmed and “fixed” regardless of a patient’s intrinsic rhythm. This method can be unsafe when used inappropriately due to the “R on T phenomena” because it can lead to ventricular fibrillation.
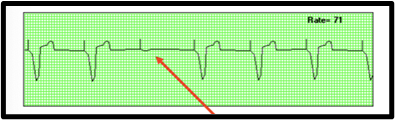
Failure to Sense
Failure to SENSE is a type of pacemaker failure when a pacemaker spike occurs where it shouldn’t be. AKA…the pacemaker has failed to sense the patient’s underlying intrinsic rhythm. Some potential causes include: the positioning of the lead, battery failure, and improper settings.

Here is what you can do:
- Assess sensitivity threshold–the mV may be too high
- Change the battery
- Assess catheter position
Failure to Capture
Failure to CAPTURE is a type of pacemaker failure where a pacing spike occurs but nothing follows. Some potential causes are: improper patient positioning, battery failure, low voltage, inadequate connection, and fibrosis of the catheter tip.
Here is what you can do:
- Increase the mA 10% above capture threshold to give a safety margin
- Reposition the patient
- Change the battery
- Reposition the catheter (need an MD for this)
- Check labs
Failure to Pace
Failure to PACE is a pacemaker failure where pacemaker spikes are “missing” or do not occur at all. Some potential causes of this are: device issues (battery failure), lead dislodgement, or pad dislodgement.

Here is what you can do:
- Assess the connections/pad adherence
- Ensure device is plugged in
- Get a new device
- Start CPR if needed
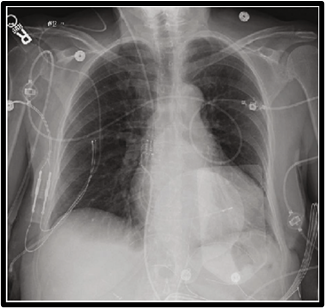
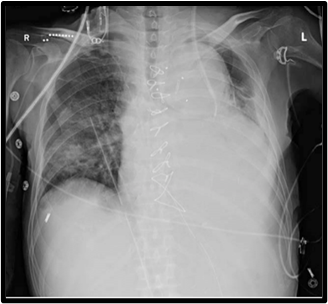
Transvenous Pacing

Transvenous pacing is another type of emergent, temporary pacing you may come across. The pacing electrode is inserted through a vein and balloon-guided to the right ventricle. Transvenous pacers can be inserted at the bedside or in the cath lab. The right IJ is the preferred insertion site but the femoral vein or left subclavian may also be used.
Initial settings for transvenous pacing are typically:
- Rate: 60-80ish bpm
- Current (output): 5-10 mA is safe
- Mode: VVI
- Sensitivity: 2ish mV is safe
It is important to keep in mind that patients may need a higher energy (mA) in acidosis, electrolyte imbalances, or if the transvenous pacer has been in for a few days.
Proper Nursing Care for Transvenous Pacing
When caring for a patient with a transvenous pacemaker, it is important to keep the following in mind:
- Immobilize affected extremity
- Monitor extremity distal to insertion site
- Possible bed rest
- Daily chest x-ray
- Do not bolus fluids through the introducer
- Monitor for signs of perforation
Hiccups with Pacemaker
If your patient ever has relentless hiccups with a cardiac pacing device, this needs to be taken seriously. Hiccups after cardiac pacemaker placement should raise concern for diaphragmatic pacing and lead perforation. This is a rare complication, but has the potential to be very lethal.
So…fun fact! If your patient keeps having hiccups…take them seriously and notify the provider!
Epicardial Pacing

Epicardial pacing is typically used in post-cardiac surgery patients, especially those who are coming off of bypass. These patients are at increased risk for arrhythmias, which are a major cause of mortality and morbidity after cardiac surgery. Temporary epicardial pacemakers have evolved from one-chamber systems to dual chamber, biatrial, and even biventricular systems!
A few tidbits to keep in mind:
- The (-) lead is used to pace, while the (+) lead is the “ground” lead
- Ventricular wires exit skin on the left
- Atrial wires exit skin on the right
Stimulation (Energy) Threshold vs Sensing Threshold
Let’s chat about stimulation vs sensing thresholds. These two concepts are often very confusing for nurses, but they are SUPER important to comprehend when it comes to managing a temporary pacemaker.

Stimulation = ENERGY
The goal with the stimulation threshold is to use the least amount of energy as possible, but still capture pacing stimulus (mA’s should be 2-3x higher than the threshold)
Sensing = VISION
The goal in sensing is to prevent competitive pacing and pace when it’s supposed to! (mV’s should be ½ the threshold value)
It is important to note that thresholds are only assessed if the patient has an underlying rhythm and is hemodynamically stable.


Add comment